Mission for Addressing and Managing Sickle Cell Disease in Nandurbar

Mission for Addressing and Managing Sickle Cell Disease in Nandurbar
Problem
- High sickle cell disease prevalence remains hidden in tribal communities
- Low diagnosis rates, late identification and limited treatment access
- Weak follow-up systems and inadequate data platforms
- Affected individuals lack access to social support schemes and entitlements
Solution
- Conducted community awareness, baseline surveys and cluster mapping in high-risk tribal regions
- Introduced mass screening through DBS and point-of-care diagnostic methods
- Strengthened laboratory capacity and trained health workers for diagnosis and treatment
- Established patient support groups and implemented a digital e-Suchi follow-up system
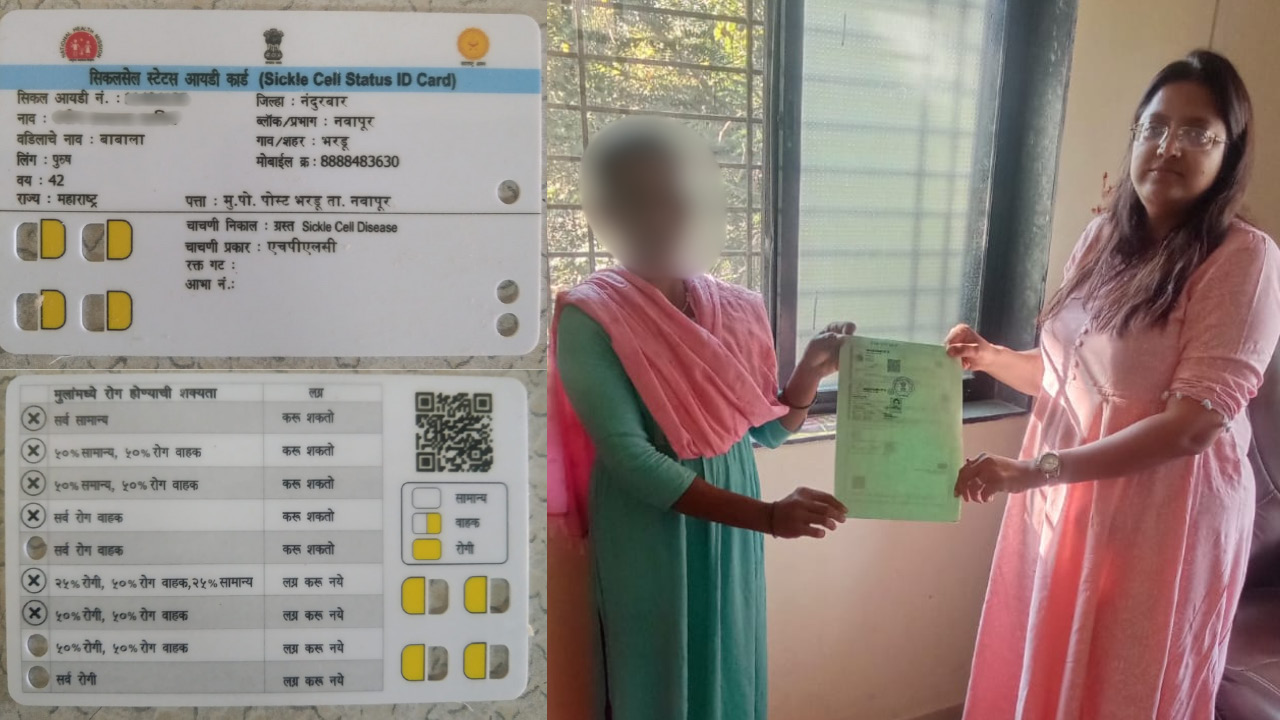
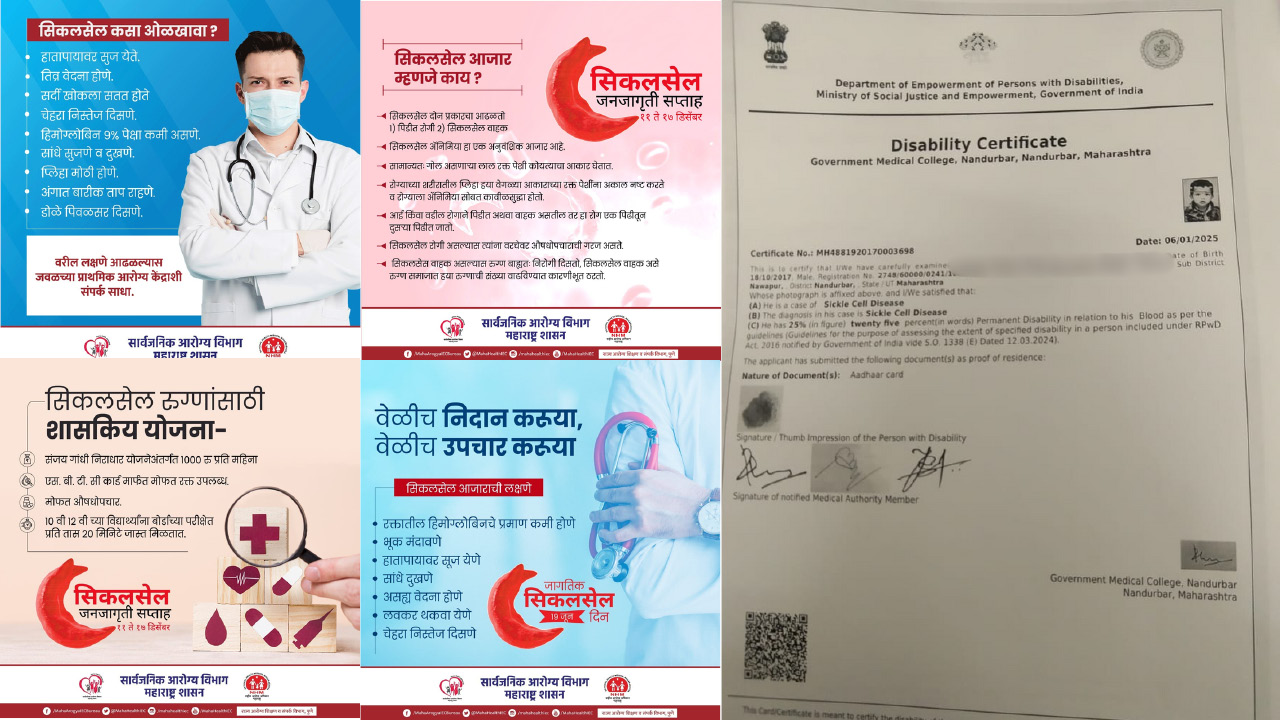
- Integrated therapy access, counselling, disability certification and welfare entitlements
Outcomes
- A total of 3,47,559 individuals were screened
- Identification of 2,566 patients and 11,655 carriers
- Almost 60% of eligible cases began Hydroxyurea therapy
- The project issued 527 disability certificates, provided 413 welfare entitlements and established seven patient support groups
- The digital e-Suchi system supports screening, monitoring and tracking of treatment
Project Details
Category: Healthcare
Project Title: Mission for Addressing and Managing Sickle Cell Disease in Nandurbar
Department or District: Public Health Department, Government of Maharashtra
State: Maharashtra
Start Date of the Project: 01-01-2024
Website: https://phd.maharashtra.gov.in/
Tribe(s) that the Project Covers: The Mission for Addressing and Management of Sickle Cell Disease in Nandurbar primarily covers tribal communities residing in the Nandurbar district of Maharashtra. The district has a very high proportion of the Scheduled Tribe population across blocks such as Akkalkuwa, Akrani, Taloda, Shahada, Navapur and Nandurbar. The disease burden is particularly concentrated among tribal groups, including Bhils, Pawaras, Madias, Pardhans and Otkars, who are known to have a high prevalence of the sickle gene. The project, therefore, focuses on vulnerable tribal populations living in remote, forested and difficult-to-reach areas.
Keywords: Sickle Cell Disease (SCD), Tribal Health, Universal Screening, Dry Blood Spot (DBS), Hydroxyurea Therapy, Genetic Counselling, e-Suchi Digital Platform, Patient Support Groups, Disability Certification, District Governance, NHM, Health Equity
Nandurbar district faces a disproportionately high burden of Sickle Cell Disease (SCD), particularly among its tribal population. Recognised as one of the ten priority health issues in tribal communities, SCD contributes significantly to childhood morbidity, mortality, maternal risk and socio-economic vulnerability. In response, the Public Health Department, Government of Maharashtra, under the leadership of the District Collector, launched a focused district-level initiative aligned with the National Sickle Cell Anaemia Elimination Mission (NHM).
The mission began on 01-01-2024, evolving into an integrated public health model that features early detection, decentralised treatment, social welfare integration, digital tracking and community engagement. Screening identified 2,566 patients and 11,655 carriers, demonstrating strong district governance and multi-sectoral collaboration.
The Project
The project is a district-led, multi-sectoral Sickle Cell Disease Elimination Mission aimed at reducing morbidity and mortality, as well as the intergenerational transmission of SCD in Nandurbar. The intervention was designed to move beyond fragmented testing efforts and create a comprehensive ecosystem that integrates screening, diagnosis, treatment, counselling, welfare entitlements and digital monitoring.
Earlier screening efforts were costly, non-exhaustive and neglected newborn and antenatal tracking. Treatment relied primarily on folic acid and Hydroxyurea was available only at higher facilities. Counselling was limited and often conducted in non-tribal languages. There was no systematic mechanism for patient identification or follow-up.
The new mission introduced Dry Blood Spot (DBS) molecular testing, decentralised Hydroxyurea availability at PHC and Sub-Centre levels, patient support systems, disability certification, pension linkages and digital monitoring through the e-Suchi platform.
Problems that it Intends to Solve
The project addresses the high prevalence and the undetected burden of sickle cell disease in tribal communities. Diagnosis rates were low and identification of carriers and patients was often delayed. Remote geography limited access to effective treatment and monitoring. Weak follow-up systems and inadequate data platforms compromised continuity of care. Additionally, affected individuals often lacked access to disability certification and welfare entitlements, deepening socio-economic distress.
Need and Rationale
SCD is a hereditary, lifelong disorder that disproportionately affects tribal populations. Without early detection and continuous management, children suffer recurrent pain crises, infections and life-threatening complications. The hereditary nature of the disease perpetuates intergenerational vulnerability. Addressing SCD is critical not only for reducing preventable deaths but also for breaking cycles of poverty, stigma and exclusion.
The mission aligns with the Government of India’s goal to eliminate SCD by 2047 and serves as a district-level operationalisation of this national vision. Early screening, genetic counselling and decentralised therapy significantly reduce long-term disease burden and healthcare costs while improving productivity and quality of life.
Implementation Process
The mission began with baseline surveys, high-risk cluster mapping and community mobilisation across schools and tribal hamlets. Mass screening was implemented using cost-effective Dry Blood Spot testing and point-of-care diagnostics, replacing earlier, expensive and limited methods.
Laboratory capacity was strengthened and Medical Officers, Community Health Officers, ASHAs and ANMs were trained to ensure standardised diagnosis and treatment. Hydroxyurea therapy was decentralised to Primary Health Centres and Sub-Centres, improving accessibility.
The digital e-Suchi platform was introduced for screening, treatment tracking and follow-up monitoring. A district helpline and control room were established to track adherence, monitor side effects and reconnect patients who missed visits. Monthly “Sickle Mela” camps were organised for follow-up testing, counselling, pension facilitation and disability certification.
Applications are first scrutinised by an Internal Scrutiny Committee within the Directorate of Tribal Welfare. Applicants are then referred to the Department of Obstetrics and Gynecology for medical examination and confirmation of genuine infertility.
Solutions Implemented
The mission introduced universal screening for individuals aged 0-40 years, in line with national operational guidelines. By the end of the evaluation period, 3,47,559 individuals were screened, resulting in the identification of 2,566 patients and 11,655 carriers.
Hydroxyurea therapy was made available at the PHC level, enabling nearly 60 percent of eligible patients to receive treatment. This decentralisation significantly reduced travel burden and improved compliance. Pain management, blood transfusion access and continuous CBC monitoring were integrated into routine services.
Seven patient support groups were established to strengthen adherence, counselling and peer engagement. Genetic counselling and marriage counselling were introduced to prevent new cases and promote informed decision-making.
The project also integrated welfare entitlements, issuing 527 disability certificates and facilitating 413 welfare scheme benefits. Integration with the Sanjay Gandhi Niradhar Scheme ensured pension access for Below Poverty Line patients. These measures ensured holistic support beyond clinical care.
The Nandurbar Sickle Cell Disease Mission implemented a comprehensive, district-wide, end-to-end intervention model that coordinated screening, diagnosis, treatment, counselling, follow-up and social welfare integration.
The first major solution was the shift to mass, universal screening using Dry Blood Spot (DBS) molecular testing, replacing earlier expensive and limited HPLC-based testing. DBS-enabled on-site sample collection, even in remote tribal hamlets, reduced diagnostic costs by approximately 75 percent, making screening scalable and sustainable. Screening was expanded to include newborns, antenatal mothers, school children and family members to interrupt intergenerational transmission.
The second major intervention was decentralisation of treatment services. Earlier, Hydroxyurea was available only at higher-level facilities. The mission ensured the availability of Hydroxyurea at Primary Health Centres and Sub-Centres with trained Medical Officers. This significantly reduced travel burden for tribal families and improved continuity of care. Pain management protocols, CBC monitoring, transfusion referral systems and follow-up schedules were institutionalised at peripheral facilities.
The third pillar was the establishment of a digital patient-tracking ecosystem via the e-Suchi platform. This system created a district repository of screened individuals, tracked disease status (TT/diseased and AT/carriers), monitored therapy initiation and flagged missed follow-ups. The digital layer converted episodic care into a longitudinal patient management system.
The fourth solution focused on community-based patient support structures. Seven patient support groups were formed to encourage peer engagement, counselling, adherence to Hydroxyurea therapy and shared learning. Marriage counselling and genetic counselling were integrated to prevent new cases and empower informed decision-making.
Finally, the project integrated social welfare convergence into the health response. Affected individuals were supported in obtaining disability certificates, travel concession cards and access to schemes such as the Sanjay Gandhi Niradhar pension. Monthly “Sickle Melas” were institutionalised to provide clinical review, counselling, pension facilitation and administrative support under one roof. This ensured that SCD care moved beyond medical management to comprehensive social protection.
Details of the Coverage
The mission targeted a district population of 11,17,845 individuals, with expected carriers of 1,11,785 and diseased individuals estimated at 11,179. During the evaluation period, 3,47,559 individuals were screened. Internal beneficiaries included 885 health personnel strengthened under the programme, while external beneficiaries exceeded 3.47 lakh screened individuals.
Innovation and Unique Features
The project’s primary innovation lies in its integrated district governance approach. It replaced costly HPLC-based centralised testing with cost-effective DBS molecular testing, reducing costs by approximately 75 percent and enabling on-site screening. The inclusion of newborn, antenatal and family tracking expanded preventive coverage.
The digital e-Suchi platform enabled real-time tracking of patient status, treatment adherence and follow-up. The helpline system proactively monitored therapy adherence and side effects, reducing default rates.
Monthly Sickle Melas institutionalised a community-centric model combining clinical follow-up, counselling, welfare access and administrative services under one platform. The integration of disability certification, travel concession cards and pension schemes made the mission socially responsive rather than purely medical.
Strong administrative leadership by the District Collector and the District Health Officer ensured convergence across health, social welfare and community institutions. This convergence-driven, digitally enabled and culturally contextualised approach sets it apart from conventional disease-control programs.
The mission stands out for integrating medical science, district governance, digital systems and social inclusion into a unified public health framework.
One of the most significant innovations was the transition to cost-effective DBS molecular screening at scale. This not only reduced costs but also enabled saturation-based screening in geographically difficult tribal areas. By targeting the 0–40 age group in alignment with national guidelines, the district adopted a preventive life-cycle approach rather than reactive treatment.
The e-Suchi digital monitoring system transformed SCD management from paper-based records into real-time, actionable data governance. Integration of screening records, therapy tracking and follow-up alerts strengthened accountability at the PHC and district levels. The district helpline and control room further enhanced digital governance by proactively calling patients to monitor adherence, check side effects and reconnect defaulters.
Another innovation was the convergence model under district leadership. The District Collector and District Health Officer institutionalised coordination across NHM, welfare departments, PHCs, NGOs and technical partners. This ensured rapid administrative decisions, resource mobilisation and adaptive management.
The introduction of Monthly Sickle Melas as a fixed institutional mechanism was also innovative. These melas combined clinical monitoring, disability certification processing, pension enrolment and counselling services into a single accessible event, reducing fragmentation and improving trust in the system.
Culturally contextualised counselling in local languages, along with the engagement of tribal influencers, addressed stigma and behavioural barriers. By embedding social security measures within the health programme, the district reframed SCD management as a dignity-driven intervention rather than a purely biomedical initiative.
Challenges Faced
Implementation was challenged by difficult terrain and remote tribal settlements, limiting access to screening and follow-up. Primary Health Centres initially lacked technical capacity and infrastructure. Social stigma and low awareness hindered care-seeking behaviour. Ensuring long-term therapy compliance among mobile tribal families required continuous engagement. Sustained funding and intersectoral collaboration were also necessary for scaling impact.
Outcomes
The mission screened over 3,47,559 individuals and identified 2,566 patients and 11,655 carriers. Approximately 60 percent of eligible patients were initiated on Hydroxyurea therapy. Seven patient support groups enhanced treatment compliance. 527 disability certificates and 413 welfare entitlements were issued, promoting social inclusion. The digital e-Suchi platform institutionalised systematic tracking and monitoring, strengthening continuity of care.
The mission achieved measurable, multidimensional outcomes across screening, treatment, digital governance and social inclusion.
During the evaluation period, 3,47,559 individuals were screened, resulting in the identification of 2,566 patients and 11,655 carriers. This represents a substantial increase in detection coverage in a previously under-diagnosed district. Early identification of carriers enables preventive counselling and long-term reduction of new cases.
Approximately 60 percent of eligible patients were initiated on Hydroxyurea therapy. Decentralisation to the PHC level improved accessibility and adherence, reducing pain crises and complications. The availability of treatment closer to home reduced catastrophic expenditures and travel hardships for tribal families.
Social inclusion outcomes were equally significant. The issuance of 527 disability certificates and the facilitation of 413 welfare entitlements ensured that patients accessed financial and administrative support. Integration with pension schemes strengthened economic resilience among Below Poverty Line households.